|
Prevalence and Determinants of Cesarean Delivery among Married Women in the Coastal Region of Bangladesh
Nishana Afrin Nishu1*,Shahinur Akter1,2,and Mosammat Rowshan Ara1
1Sociology Discipline, Social Science School, Khulna University, Khulna 9208, Bangladesh 2Faculty of Social Sciences, Chiang Mai University, Chiang Mai 50200, Thailand. |
|
Keywords |
|
Abstract |
|
Cesarean delivery; Prevalence; Determinants; Married women; Coastal Bangladesh. |
|
This study investigated the prevalence and determinants of caesarean section (CS) delivery among married women in selected coastal areas of Bangladesh. A community-based cross-sectional study was carried out in two villages of Bagerhat and Khulna districts. Data were collected from 400 married women of at least one child under five years through simple random sampling. Findings depicted that the prevalence of CS delivery was 37.3%. Multivariate analysis revealed husband’s education and place of delivery were the significant determinants of CS delivery. Married women whose husbands had primary education (AOR = 0.019; 95% CI: 0.001-0.529; p = 0.020) and those who delivered at home had significantly lower odds of CS delivery (AOR = 0.002; 95% CI: 0.000-0.030; p < 0.001) compared to those whose husbands were non-literate and those delivered at hospital or clinics. Based on the findings, the study recommends engaging husbands particularly by improving male educational attainment to reduce unnecessary CS deliveries. Besides, at the health-system level, it calls for targeted institutional policies and the implementation of rigorous clinical audit mechanism to monitor indications and promote evidence-based obstetric practice. |
Introduction
Caesarean section (CS) delivery is typically performed to address urgent obstetric emergencies and to optimize health outcomes for both mothers and their newborns (Khan et al., 2022). Nonetheless, the world has witnessed an influx in CS delivery rates over recent decades, with recent data from the World Health Organization (WHO) indicating that CS now represents 1 in 5 childbirths (World Health Organization, 2021). The number of births by caesarean delivery was 16 million in 2000, accounting 12.1% of all live births, and within two decades, this figure increased to 29.7 million, representing 21.1% of all live births in 2021 (Betran et al., 2021). It is expected that CS delivery rate will continue climbing over the next decade, with projections suggesting that by 2030, nearly a third (29%) of all births could be performed by CS delivery (World Health Organization, 2021, Betran et al., 2021). Low- and middle-income countries (LMIC) are anticipated to see 33.5 million CS deliveries by 2030 (Betran et al., 2021). Like other LMIC, Bangladesh experienced a rise in the proportion of CS deliveries from 4% to 23% between 2004 and 2014 (Mia et al., 2019). The CS delivery rate in Bangladesh has dramatically increased, positioning it among the nations with the highest caesarean delivery rates globally, with the Bangladesh Demographic and Health Survey (BDHS) 2022 reporting it at 44% (National Institute of Population Research and Training (NIPORT) and ICF, 2024), which is three times higher compared to the WHO’s recommended standard rate of 10%-15% (Sandall et al., 2018, Mia et al., 2019). Similarly, the rate of CS in Bangladesh is among the highest in South Asia (Rana et al., 2024). The prevalence of CS delivery in rural Bangladesh has been rising steadily, reaching 40.2% according to the most recent BDHS 2022 (National Institute of Population Research and Training (NIPORT) and ICF, 2024). This upward trend is particularly striking given the traditionally limited access to advanced obstetric care in rural areas and underscores a growing shift in delivery practices. Several factors may account for this escalation. Expanding rural health infrastructure and the proliferation of private clinics have increased the availability of surgical obstetric services, while improved transportation networks facilitate access to facility-based care. Simultaneously, heightened awareness of potential complications and a perception of greater safety in surgical births may lead families to prefer CS, even when not medically indicated. Profit-driven incentives within the private healthcare sector further contribute to the overuse of CS, as facilities and providers may benefit financially from performing surgical deliveries (Hoxha et al., 2017, Cavallaro et al., 2013). It has evident that some physicians conduct CS for economic gains without any medical justification (RadhakrishnanVasanthakumari and Babu, 2017). Given the above discussion, it is therefore essential to identify the trends and the most important determinants and their influence on CS deliveries in southwestern coastal areas of Bangladesh. Existing research documented several demographic and socioeconomic factors linked to CS delivery in Bangladesh. Key factors include maternal age, age at first birth, number of antenatal visits, women’s education, employment status, and body mass index (BMI), as well as husband’s education, household wealth, and geographic location (Abdulla et al., 2023, Kumar and Sharma, 2023, Rahman et al., 2018). Additional influences such as place of residence, religious affiliation, and family size have also been shown to shape CS delivery (Hasan et al., 2020, Rahman et al., 2018, AhmmedManik and Hossain, 2021). Evidence further suggests that employed women are more likely to undergo CS than those who are unemployed (Morris et al., 2012), while higher socioeconomic status and higher maternal education increase the likelihood of choosing a surgical birth (Abdulla et al., 2023). Furthermore, delivery in private clinics is strongly associated with higher CS rates (Rahman et al., 2018). Beyond structural and economic drivers, psychological factors including limited knowledge about natural childbirth (Azami-Aghdash et al., 2014) and heightened fear, anxiety, or anticipation of labor pain have been reported as additional motivators for opting for CS delivery (Monari et al., 2008). In Bangladesh, CS deliveries are frequently performed without clear medical indication, exposing mothers and infants to both immediate and prolonged health risks (HasanAlam and Hossain, 2019). The elevated CS rates are associated with serious maternal complications including postpartum haemorrhage, infections, and even mortality (Betran et al., 2016) as well as substantial financial burdens for families (Betran et al., 2016, Kumar and Sharma, 2023). Infants born via unnecessary CS face heightened risks of brain injury, prematurity, respiratory distress, and procedure-related trauma (Betran et al., 2016, Kumar and Sharma, 2023, Shirzad et al., 2019). To mitigate the adverse effects of CS on mothers and newborns, it is imperative to identify the underlying determinants of CS delivery in the context of rural and coastal Bangladesh to inform policies and interventions that protect maternal and neonatal health.
Although several studies have examined CS delivery in Bangladesh, the majority have relied on secondary analyses of BDHS data (Abdulla et al., 2023, KhanIslam and Akter, 2023, Kumar and Sharma, 2023, Rahman et al., 2018, Kundu et al., 2024). However, there remains a substantial research gap regarding the unique dynamics of CS delivery within coastal areas of Bangladesh. Addressing this gap necessitates community-based research capable of capturing the lived realities of coastal populations and generating context-specific insights essential for locally tailored policies and interventions to curb the rate of CS delivery in these vulnerable, hard-to-reach communities of Bangladesh. Thus, this study aims to address the following research questions:
The need is underscored by the southwestern districts of Khulna and Bagerhat of Khulna division, which have experienced one of the fastest national increases in CS, with BDHS 2022 reporting a prevalence of 66% (National Institute of Population Research and Training (NIPORT) and ICF, 2024). To fill this critical gap, the present investigation provides the first community-based assessment of CS prevalence and its determinants in these coastal areas, offering context-specific insights to inform policies aimed at reducing unnecessary surgical births.
Literature Review
CS delivery rate has risen sharply in Bangladesh over the past two decades, driven by complex social, clinical, and health-system factors. National survey data indicate a marked upward trend in facility and population-level CS use, prompting concern about medically unnecessary procedures and their public-health consequences. The recent BDHS 2022 documented this rapid increase and regional variations in CS prevalence, highlighting high-burden areas that warrant closer examination (National Institute of Population Research and Training (NIPORT) and ICF, 2024).
Global and regional patterns and trends
Global evidence demonstrates a steep and sustained rise in CS rates over the past two decades (Chongsuvivatwong et al., 2010), much of it attributed to non-medical indications (Aminu et al., 2014). Approximately one-third of the 18.5 million CS deliveries conducted annually worldwide are considered unnecessary (Lavender et al., 2012), and the global proportion of births delivered by CS is projected to reach roughly 28% by 2030 (Betran et al., 2021). Developed countries drive much of this growth, such as in the United States, CS rates climbed from 5% in 1970 to 31.9% in 2016, making it the most common major surgical procedure among women (Sung et al., 2025). Latin America shows similarly elevated level, with Brazil reporting CS rates of around 56% (Pires et al., 2023) and nearly half of all births (46.4%) delivered surgically between 1994 and 2019 (PiresLeal and Silva, 2025). By contrast, Sub-Saharan Africa remains far lower at around 5% (Betrán et al., 2016), with India reporting at 17.2% (Bhatia et al., 2020) and Pakistan at 19.6% (Amjad et al., 2020) respectively. Regionally, Latin America and the Caribbean have the highest average prevalence (32%), whereas Africa reported the lowest rate (7%) (Betran et al., 2021). Bangladesh has also witnessed a sharp escalation in CS deliveries. National surveys show CS prevalence rising from 2.7% in 2001 to 44% in 2022 (Mazzoni et al., 2011, National Institute of Population Research and Training (NIPORT) and ICF, 2024). The latest BDHS 2022 reported the regional variations in CS rates as the highest reported in Khulna division (66%), followed by Rajshahi (53.6%) and Dhaka division (53.1%), while the lowest prevalence in Sylhet (25.7%) and Chittagong division (31%) (National Institute of Population Research and Training (NIPORT) and ICF, 2024). Moreover, several recent studies report that CS prevalence is concentrated among urban and wealthier groups but is also increasing in rural settings (National Institute of Population Research and Training (NIPORT) and ICF, 2024, Abdulla et al., 2023, Sujon et al., 2025, Kundu et al., 2024). These spatial and socioeconomic disparities underscore the need to examine local contexts particularly coastal and hard-to-reach areas where service access, cultural norms, and economic constraints may interact differently with CS use.
Determinants of CS delivery
Socioeconomic and demographic factors
Existing research links maternal and household socioeconomic status to the likelihood of CS. Maternal education, household wealth, and employment status have been repeatedly associated with higher CS rates, often illustrated as greater ability to access and afford facility-based obstetric care or as a preference for surgical delivery among more educated and affluent families (Sujon et al., 2025, Abdulla et al., 2023, Rahman et al., 2018). Maternal age, parity, and body mass index (BMI) are also reported as individual-level predictors of CS (Khan et al., 2017, Abdulla et al., 2023, Ireen et al., 2024). Higher maternal age increases the likelihood of CS birth (Rahman et al., 2014).
Health service and institutional factors
Health-system factors are pivotal in explaining rising CS rates. Facility type (private vs. public), availability of skilled birth attendants and specialist clinicians, and facility capacity for emergency obstetric surgery shape both access and the propensity to perform CS (Manasyan et al., 2019, Jenabi et al., 2020, Ireen et al., 2024). Several studies have highlighted the role of private facilities, where financial incentives and differing clinical practices may drive CS proportions, while facility births attended and by skilled providers are more likely to result in CS delivery than home births attended by unskilled attendants (Abdulla et al., 2023, AhmmedManik and Hossain, 2021).
Clinical and obstetric factors
Clinical indications and pregnancy characteristics including pregnancy complications, preterm delivery, and fetal distress remain core determinants of medically necessary CS (Rahman et al., 2018, Tayaba et al., 2024). A prior study suggests that pregnancies at advanced maternal ages are associated with several biological changes, including malposition of the fetus and a higher risk of complications such as hypertension, eclampsia, and diabetes (Ireen et al., 2024), which increased the risk for CS.
Psychosocial and information-related factors
Knowledge, perceptions, and fear of labor pain also influence delivery mode. Limited knowledge about the risks and benefits of vaginal versus surgical birth, together with community norms and mass-media messaging, affect women’s preferences and readiness to seek CS delivery (Azami-Aghdash et al., 2014, Monari et al., 2008). Exposure to mass media and antenatal counseling are associated with a greater propensity for CS delivery (Ireen et al., 2024). Nowadays, many educated pregnant women in Bangladesh prefer to avoid vaginal delivery due to fear of labor pain and potential complications, which largely contributes to the rising CS rates (HasanAlam and Hossain, 2019).
Research gaps and justification for the current study
While numerous studies have examined the factors influencing CS delivery, the literature shows two important gaps. First, most large-scale analyses rely on BDHS secondary data, which reveal national trends but offer limited insight into local contextual factors, provider incentives, or community-level experiences. Second, coastal regions characterized by environmental vulnerability, infrastructural constraints, and distinctive livelihood patterns (Nishu et al., 2025, Akter et al., 2023) have received limited primary, community-based investigation, despite evidence of sharply rising CS rates in some southwestern districts (Kundu et al., 2024). Addressing this gap requires geographically focused research capable of disentangling how coastal-specific barriers, cultural norms, and facility practices jointly determine CS utilization. Such community-based primary data are essential for generating actionable and context-sensitive policy recommendations.
Conceptual framework
Figure 1. Conceptual framework of the determinants of caesarean section (CS) delivery
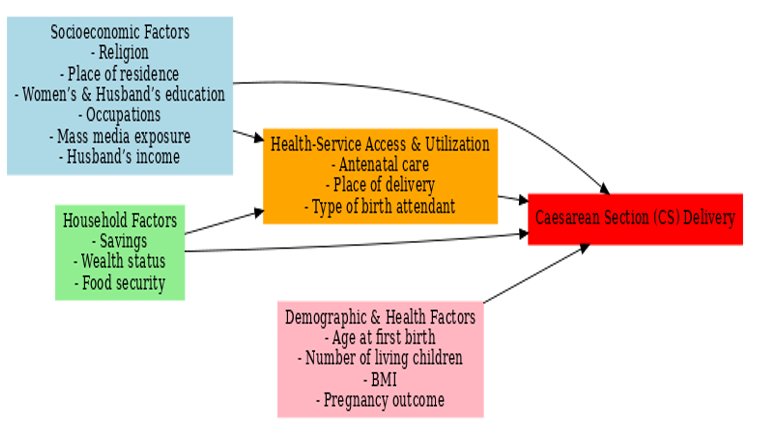
Figure 1 illustrates the conceptual pathways through which socioeconomic, household, demographic and health factors shape the likelihood of CS delivery. Socioeconomic and household factors influence access to and utilization of maternal health services such as antenatal care, delivery settings, and skilled birth attendance, which mediate their effects on CS delivery. Demographic and health-related factors exert both direct and indirect influences on the likelihood of CS delivery.
Methods and Materials
Study area
This cross-sectional study was conducted following survey method to systematically collect and analyze quantitative data, offering a clear understanding of the determinants of CS delivery among married women in the study area. This method is particularly appropriate for capturing attitudes, perceptions, and behaviors within a defined population over a short period (Akter et al., 2023) and facilitates rapid, evidence-based investigation and knowledge generation (AkterRahman and Razu, 2020). The study was conducted in Khulna and Bagerhat districts of Khulna division, which were selected due to its highest prevalence rate of CS deliveries, reported at 66% in the BDHS 2022 (National Institute of Population Research and Training (NIPORT) and ICF, 2024). Two coastal villages namely Joymoni in Mongla upazila of Bagerhat district and Sutarkhali village in Dacope upazila of Khulna district of Bangladesh were selected as the study sites because their geographic, socioeconomic, and environmental conditions make them particularly relevant for examining the prevalence and determinants of CS delivery among married women. These low-lying coastal areas are highly vulnerable to salinity intrusion, cyclones, and recurrent flooding, which disrupt livelihoods, constrain healthcare infrastructure (Nishu et al., 2025), and limit access to skilled maternal care. Women in these settings often face compound barriers such as poverty, transportation challenges, and limited availability of obstetric services, all of which can influence both the demand for and the necessity of CS deliveries. Furthermore, cultural practices and health-seeking behaviors in these isolated communities may differ from those in other regions of Bangladesh (Akter et al., 2023), providing unique insights into how environmental stressors and social determinants shape maternal health outcomes. Importantly, no prior research has specifically investigated CS delivery in these coastal contexts, underscoring the significance of focusing on these villages to fill a critical evidence gap and inform targeted maternal health interventions.
Sample and sampling
The respondents for this study were chosen based on specific eligibility criteria to ensure that the findings accurately reflect the target population. The participants were the married women who had at least one child under the age of five and had maintained continuous residence in the study area for a minimum of three years. These criteria were applied to capture women with recent childbirth experience while also ensuring a stable population, thereby minimizing recall bias and the influence of temporary migration. In May 2023, a household census was conducted to gather information about the population that met the criteria for participation. According to the census, the total population consisted of 1,198 married women. The required sample size was determined using Cochran’s random sampling formula, which yielded a minimum sample size of 400 mothers was based on 95% confidence level and 5% margin of error (Cochran, 1977). Finally, simple random sampling was employed to select participants from the census list. This method was chosen to give every eligible woman an equal chance of inclusion, thereby minimizing selection bias and enhancing the external validity of the results. Such a rigorous and transparent sampling strategy strengthens the representativeness of the data and the credibility of subsequent analyses.
Measures Socioeconomic profile
Socioeconomic profile encompasses factors such as residence (Joymuni and Sutharkhali village), religion (Muslim and non-Muslim), women’s educational status (Non-literate, primary, secondary, and tertiary), women’s occupational status (Not working and working), mass media exposure (No/yes), educational attainment of husbands (Non-literate, primary, secondary and tertiary), occupation of husbands (business, self-employed, day labor, employee and others), and monthly income of husbands (Bangladeshi Taka [BDT] ≤ 10,000, 10,001-20,000, and ≥ 20,001).
Demographic and health-related factors
Demographic factors include age at first birth (< 18 years, 18-22 years, and ≥ 23 years), and number of living children (1, 2, and ≥ 3). Health-related factors focus on women’s BMI (Underweight [< 18.5], normal weight [18.5-24.9], overweight and obesity [ ≥ 25.0]) (World Health Organization, 2010), receiving antenatal care during pregnancy (No/yes), place of delivery (Hospital/clinic, home), type of birth attendant (Unskilled [dai] and skilled), and pregnancy outcome (Preterm/term).
Household information
Household information includes household savings, wealth and food insecurity. Households’ monthly savings were classified into no savings, BDT ≤ 1000, ≥ 1,001. The assessment of household wealth was conducted based on a wealth index comprising 27 items used in the BDHS (National Institute of Population Research and Training, 2020), measured on a dichotomized scale of yes = 1 and no = 0. Subsequently, the household wealth index was categorized into low (1-6), moderate (7-11) and high (12-16) levels. The household food insecurity access scale (index), developed by CoatesSwindale and Bilinsky (2007) was employed to measure household food insecurity. This was then classified into food secure, mild food insecure, moderately food insecure, and severely food insecure household.
Data collection and analysis
Data were collected through a semi-structured interview schedule between July and August 2023. The interview schedule consisted of eight distinct sections addressing various topics such as demographic, socioeconomic, household, and health-related information. Researchers and their associates collected data at the household level utilizing a replacement method. Statistical Packages for the Social Sciences (SPSS) version 21 was used to analyze the data. Percentage analysis was conducted to assess the prevalence of CS delivery among married women. Pearson’s χ2 test and Fisher’s exact test were conducted to identify the factors associated with the prevalence of CS delivery among women. Consequently, the significant variables extracted from bivariate analyses were used to conduct binary logistic regression analysis (p < 0.10). Multivariate logistic regression results were presented by adjusted odds ratios (AOR) with 95% confidence intervals (CI) and the significance level of p < 0.05.
Ethical approval
Ethical approval was obtained from the Ethical Clearance Committee of Khulna University, with reference number KUECC-2023-07-37. Additionally, informed verbal consent was secured from the participants. The respondents were guaranteed that all the information would be kept confidential and used solely for research purposes.
Results
Prevalence of caesarean delivery
Table 1 shows that the prevalence of CS delivery was 37.3% among married women in the coastal study population, while the majority had normal delivery (62.8%).
Table 1. Prevalence of caesarean delivery
| Type of delivery (n=400) | Frequency | Percent (%) |
|---|---|---|
| Normal | 251 | 62.8 |
| Caesarean | 149 | 37.3 |
Bivariate association of the type of delivery and its associated factors
Table 2 presents the bivariate associations examining factors associated with CS delivery among married women in two coastal villages of Bangladesh. Findings revealed that several socioeconomic characteristics demonstrated significant associations. Religion was significantly associated with CS delivery among married women (p < 0.001) reporting higher prevalence of CS among Muslim women. Residence in Sutarkhali village was also significantly related to CS (p = 0.019). Educational attainment showed significant association, both respondents and their husbands with secondary and tertiary education had significantly higher CS than those with lower educational levels (p < 0.001 for both). Husband’s occupation was also significantly associated with CS delivery (p = 0.056). Women from households with higher monthly income (≥ 20,001 BDT) represents higher percentages of CS (p < 0.001). Respondents’ occupation (p = 0.030) and exposure to mass media was significantly associated with CS delivery (p < 0.001).
Household factors such as monthly savings, household wealth and food insecurity were significantly associated with CS delivery among married women. Women from households with any level of savings (p = 0.008), moderate or high wealth (p < 0.001) and food secure households (p = 0.008) had higher CS prevalence.
Among demographic and health-related factors, delayed childbearing and number of living children were significantly associated with CS (p < 0.001 for both). Additionally, receiving antenatal care (p < 0.001), place of delivery (p < 0.001), and skilled birth attendants were significantly related to CS deliveries (p < 0.001). Preterm pregnancies were slightly more common among CS deliveries (p = 0.035).
Table 2. Bivariate analyses of the factors associated with type of delivery
|
Variables |
Type of delivery |
p value |
Chi-square test/Fisher’s Exact test value |
||
|
Normal (%) |
Caesarean (%) |
||||
|
Socioeconomic Factors |
|
|
|
|
|
|
Religion |
|
|
|
|
|
|
|
Non-Muslim |
28 (11.2) |
55 (36.9) |
< 0.001*** |
37.721 a |
|
|
Muslim |
223 (88.8) |
94 (63.1) |
|
|
|
Place of residence |
|
|
|
|
|
|
|
Joymoni village |
140 (55.8) |
65 (43.6) |
0.019** |
5.527 a |
|
|
Sutarkhali village |
111 (44.2) |
84 (56.4) |
|
|
|
Respondent’s education |
|
|
|
|
|
|
|
Non-literate |
7 (2.8) |
1 (0.7) |
|
|
|
|
Primary |
64 (25.5) |
18 (12.1) |
< 0.001*** |
18.489b |
|
|
Secondary |
176 (70.1) |
120 (80.5) |
|
|
|
|
Tertiary |
4 (1.6) |
10 (6.7) |
|
|
|
Respondent’s occupation |
|
|
|
|
|
|
|
Non-working mother |
221 (88.0) |
141 (94.6) |
0.030** |
4.713a |
|
|
Working mother |
30 (12.0) |
8 (5.4) |
|
|
|
Exposure to mass media |
|
|
|
|
|
|
|
No |
174 (69.3) |
74 (49.7) |
< 0.001*** |
15.336 a |
|
|
Yes |
77 (30.7) |
75 (50.3) |
|
|
|
Husband’s education |
|
|
|
|
|
|
|
Non-literate |
22 (8.8) |
3 (2.0) |
< 0.001*** |
42.718 b |
|
|
Primary |
86 (34.3) |
26 (17.4) |
|
|
|
|
Secondary |
137 (54.6) |
95 (63.8) |
|
|
|
|
Tertiary |
6 (2.4) |
25 (16.8) |
|
|
|
Husband’s occupation |
|
|
|
|
|
|
|
Business |
31 (12.4) |
26 (17.4) |
0.056* |
9.053 b |
|
|
Self-employed |
82 (32.7) |
41 (27.5) |
|
|
|
|
Day labor |
114 (45.4) |
58 (38.9) |
|
|
|
|
Employee |
18 (7.2) |
22 (14.8) |
|
|
|
|
Others |
6 (2.4) |
2 (1.3) |
|
|
|
Husband’s monthly income (in BDT) |
|||||
|
|
≤ 10000 |
156 (62.2) |
68 (45.6) |
< 0.001*** |
19.153 a |
|
|
10001-20000 |
89 (35.5) |
64 (43.0) |
|
|
|
|
≥ 20001 |
6 (2.4) |
17 (11.4) |
|
|
|
Household Factors |
|||||
|
Monthly savings (in BDT) |
|
|
|
|
|
|
|
No savings |
183 (72.9) |
91 (61.1) |
0.008*** |
9.638 a |
|
|
≤ 1000 |
32 (12.7) |
18 (12.1) |
|
|
|
|
≥ 1001 |
36 (14.3) |
40 (26.8) |
|
|
|
Household wealth |
|
|
|
|
|
|
|
Low |
112 (44.6) |
42 (28.2) |
< 0.001*** |
16.476 b |
|
|
Moderate |
135 (53.8) |
96 (64.4) |
|
|
|
|
High |
4 (1.6) |
11 (7.4) |
|
|
|
Household food insecurity |
|
|
|
|
|
|
|
Food secure household |
67 (26.7) |
62 (41.6) |
0.008*** |
11.915 a |
|
|
Mildly food insecure household |
55 (21.9) |
27 (18.1) |
|
|
|
|
Moderately food insecure household |
107 (42.6) |
55 (36.9) |
|
|
|
|
Severely food insecure household |
22 (8.8) |
5 (3.4) |
|
|
|
Demographic and Health-related Factors |
|||||
|
Respondent’s age at first birth |
|
|
|
|
|
|
|
< 18 years |
103 (41.0) |
26 (17.4) |
< 0.001*** |
32.435 a |
|
|
18-22 years |
121 (48.2) |
82 (55.0) |
|
|
|
|
≥ 23 years |
27 (10.8) |
41 (27.5) |
|
|
|
Number of living children |
|
|
|
|
|
|
|
1 |
87 (34.7) |
82 (55.0) |
< 0.001*** |
21.543 a |
|
|
2 |
113 (45.0) |
57 (38.3) |
|
|
|
|
≥ 3 |
51 (20.3) |
10 (6.7) |
|
|
|
Respondent’s BMI |
|
|
|
|
|
|
|
Underweight |
34 (13.5) |
16 (10.7) |
0.361 |
2.038 a |
|
|
Normal weight |
142 (56.6) |
95 (63.8) |
|
|
|
|
Overweight and obesity |
75 (29.9) |
38 (25.5) |
|
|
|
Receiving antenatal care during pregnancy |
|
|
|
|
|
|
|
No |
35 (13.9) |
3 (2.0) |
< 0.001*** |
15.480 a |
|
|
Yes |
216 (86.1) |
146 (98.0) |
|
|
|
Place of delivery |
|
|
|
|
|
|
|
Hospitals/clinics |
24 (9.6) |
148 (99.3) |
< 0.001*** |
376.347 b |
|
|
Home |
227 (90.4) |
1 (0.7) |
|
|
|
Type of birth attendant |
|
|
|
|
|
|
|
Unskilled (dai) |
199 (79.3) |
0 (0.0) |
< 0.001*** |
298.395 b |
|
|
Skilled |
52 (20.7) |
149 (100.0) |
|
|
|
Pregnancy outcome |
|
|
|
|
|
|
|
Preterm |
35 (13.9) |
33 (22.1) |
0.035** |
4.459 a |
|
|
Term |
216 (86.1) |
116 (77.9) |
|
|
aChi-square test value b Fisher’s Exact test value ***Significant at 1% level; **Significant at 5% level; *Significant at 10% level
Multivariate analysis of the factors associated with caesarean delivery
Multivariate binary logistic regression analysis was conducted to identify the determinants of caesarean delivery. Here, type of delivery (Normal = 0 and caesarean delivery = 1) was the outcome variable, and the explanatory variables were the significant variables extracted from bivariate analyses. Results revealed that socioeconomic factors like husband’s education as well as demographic and health-related factors such as place of delivery were the significant determinants of CS delivery among women in coastal areas of Bangladesh. However, household factors had no significant association with CS delivery among women. Moreover, married women with husbands who had primary level of education have 0.019 times lower odds of CS delivery (AOR = 0.019; 95% CI: 0.001-0.529; p = 0.020) compared to women with non-literate husbands. Furthermore, married women who delivered at home have lower odds of CS delivery (AOR = 0.002; 95% CI: 0.000-0.030; p < 0.001) than those who delivered at hospitals or clinics.
Table 3. Binary logistic regression analysis of the determinants of caesarean delivery among women
| Factors | SE | P value | AOR | 95% CI (Lower–Upper) | |
|---|---|---|---|---|---|
| Socioeconomic Factors | |||||
| Husband’s education | |||||
| Non-literate (Ref) | |||||
| Primary | 1.699 | 0.020** | 0.019 | 0.001–0.529 | |
| Secondary | 1.687 | 0.755 | 0.590 | 0.022–16.123 | |
| Tertiary | 1.431 | 0.228 | 0.178 | 0.011–2.946 | |
| Demographic and Health-related Factors | |||||
| Place of delivery | |||||
| Hospitals/clinics (Ref) | |||||
| Home | 1.398 | <0.001*** | 0.002 | 0.000–0.030 | |
Ref. Reference group; SE: Standard Error; AOR: Adjusted Odd Ratio; CI: Confidence interval; ***Significant at 1% level; **Significant at 5% level
Discussion
This study aimed to investigate the prevalence and determinants of CS delivery among married women in coastal areas of Bangladesh. Findings revealed that CS prevalence of 37.3%, which is lower compared to the national prevalence rate of 44% reported in BDHS 2022 (National Institute of Population Research and Training (NIPORT) and ICF, 2024). However, this prevalence is higher compared to previous studies conducted in Bangladesh, that is 32.73% (Kundu et al., 2024, Khan et al., 2022) and is substantially higher than rates observed in neighboring countries, including Pakistan (14%), India (14%), and Nepal (4%) (Mia et al., 2019).
The relatively lower prevalence of CS delivery observed in this community-based study, compared with the national average in Bangladesh, likely reflects the contextual characteristics of the study area. The research was conducted in predominantly rural coastal areas of Bangladesh with limited healthcare infrastructure, low socioeconomic status, and prevailing cultural beliefs and practices, all of which may constrain access to facility-based deliveries and influence the observed CS delivery rates.
The significant determinants identified in this study were presented under the headings of socioeconomic, household, demographic and health-related factors for better organization of the findings.
Socioeconomic determinants
Among the socioeconomic factors, the present study identified husbands’ education level as a significant determinant of CS delivery among married women in coastal Bangladesh. Findings suggest that married women with husbands possessing primary education have lower odds of CS delivery compared to those with non-literate husbands aligns with existing literature. Several studies have highlighted the significant role of husband’ education in influencing birth-related decisions and maternal health outcomes. For instance, previous studies in Bangladesh, India, and other South Asian countries found that husbands’ educational qualifications significantly predicted the likelihood of CS delivery, with higher educational levels being associated with increased odds of opting for CS delivery (Ireen et al., 2024, Verma et al., 2020, Kumar and Dhillon, 2021, Mia et al., 2019). Similarly, Abdulla et al. (2023) indicated that women whose husbands had primary to higher education were more likely to accept CS deliveries. This finding may be interpreted by the role of husband’s educational attainment in shaping birth-related decisions, as higher education can improve health knowledge, increase awareness of pregnancy complications, and facilitate access to maternal healthcare services, particularly in resource-constrained coastal settings. These findings underscore the importance of husbands’ education in shaping maternal health decisions, suggesting that enhancing men’s educational attainment may be a strategic approach to reducing unnecessary CS deliveries.
Although previous studies documented significant associations between CS delivery with religion (Abdulla et al., 2023, Sujon et al., 2025, HasanAlam and Hossain, 2019), place of residence (Khan et al., 2017, Abdulla et al., 2023, Rana et al., 2024), women’s education (Abdulla et al., 2023, Khan et al., 2017, Rahman et al., 2018, HasanAlam and Hossain, 2019), women’s working status (Abdulla et al., 2023, Sujon et al., 2025), mass media exposure (Torloni et al., 2020, Sujon et al., 2025), and husbands occupation (Abdulla et al., 2023, Sujon et al., 2025), the present study did not identify significant relationships of CS delivery with religion, place of residence, women’s education, occupation, and exposure to mass media, husband’s occupation or income. These inconsistencies may reflect contextual differences in educational attainment, economic conditions, and sociocultural norms and beliefs across regions, which can shape maternal health behaviors and access to obstetric care.
Household determinants
Existing research have consistently demonstrated a significant association between household economic status particularly household wealth and CS delivery, with women from wealthier families more likely to undergo CS due to greater financial capacity to afford surgical procedures (Abdulla et al., 2023, Mia et al., 2019, Rahman et al., 2018, Sujon et al., 2025, Ahmed et al., 2023). In contrast, the present study found no significant relationship between CS delivery and household-level factors such as savings, wealth, or food insecurity. This divergence may reflect the distinctive context of coastal Bangladesh, where healthcare access is limited, health service utilization is hindered by geographic and infrastructural barriers and entrenched cultural or local practices may influence maternal healthcare decisions differently from those in other regions.
Demographic and health-related determinants
Among the demographic and health-related factors, the study identified place of delivery as a significant determinant of CS delivery. We found that married women who delivered at hospitals or clinics had higher odds of CS delivery than those who delivered at home, reflecting the predominance of vaginal deliveries in home settings and the higher likelihood of surgical intervention in institutional facilities. This pattern aligns with prior studies (Rowe et al., 2016, Jenabi et al., 2020, Ahmed et al., 2023). Moreover, the profit-driven nature of Bangladesh’s private health sector provides financial incentives that may encourage unnecessary caesarean deliveries. Supporting this, a study reported that women delivering in private hospitals were more than 38 times as likely to undergo CS deliveries compared to those giving birth outside institutional facilities (AhmmedManik and Hossain, 2021). There, these findings highlight the need for stronger regulatory oversight and evidence-based clinical guidelines to curb non-medically indicated CS deliveries.
Moreover, previous studies have consistently identified maternal age at first birth (Rahman et al., 2018, Janoudi et al., 2015, Khan et al., 2017), the number of living children is particularly fewer children (Khan et al., 2017), receiving antenatal care (Fabbro et al., 2022, AhmmedManik and Hossain, 2021, Khan et al., 2017), delivery attended by skilled birth attendant (Manasyan et al., 2019), and preterm pregnancy (Tayaba et al., 2024) as key determinants of CS delivery. Nonetheless, the current study found no statistically significant associations between CS delivery and women’s age at first birth, number of living children, antenatal care utilization, type of birth attendant, and pregnancy outcome.
These discrepancies may be explained by the unique sociodemographic context of the coastal study areas. Limited access to comprehensive obstetric services, coupled with infrastructural barriers and geographic isolation, may constrain opportunities for facility-based deliveries, thereby attenuating the influence of factors such as antenatal care or skilled attendance that are typically predictive of CS in urban or better-resourced settings. Additionally, entrenched cultural norms regarding home births and restricted decision-making autonomy for women may override individual demographic or health-related factors in shaping delivery, which highlights the need for further investigation in a broader context.
Strengths and Limitations
A key strength of this research lies in its community-based approach, which enabled a robust assessment of both the prevalence and determinants of CS delivery among married women in selected coastal areas of Bangladesh. This study provides locally relevant evidence that can inform targeted policies aimed at reducing unnecessary CS delivery. Additionally, the findings contribute to the broader maternal health literature by offering context-specific insights from coastal communities. However, several limitations warrant consideration. Cross-sectional design restricts causal inference, and reliance on self-reported data may introduce recall bias. The study’s focus on selected coastal areas limits the generalizability of the findings to other populations, while the exclusive use of quantitative approach constrains in-depth exploration of the underlying social, cultural, and behavioral drivers of CS delivery. Future research employing mixed methods across broader geographic settings is recommended to provide more comprehensive and nuanced insights into the determinants of CS delivery.
Conclusion
This study investigated the prevalence and determinants of CS delivery among married women in coastal areas of Bangladesh and found a prevalence of 37.3%. Multivariate analysis identified husband’s education and place of delivery as the significant determinants of caesarean delivery indicating women whose husbands had primary education and those who delivered at home were less likely to have CS delivery compared with women whose husbands were non-literate and those delivered at hospitals or clinics. Based on these findings, the study recommends that interventions should extend to actively involving husbands, with particular emphasis on raising male educational attainment as a strategy to curb unnecessary CS delivery. At the health-system level, targeted policies within healthcare institutions are warranted to reduce non-medically indicated procedures including the establishment of robust clinical audit systems to monitor CS indications and reinforce evidence-based obstetric practice. Besides, further research incorporating mixed methods (both quantitative and qualitative approaches) across diverse geographic contexts would be carried out on this issue for better generalization.
Acknowledgement
We gratefully acknowledge the Research and Innovation Centre of Khulna University, Khulna, Bangladesh, for providing financial support for this study. Besides, we also extend our sincere appreciation to the study participants for their valuable cooperation and to the data collection team for their dedicated contributions to the research process.
Literature Review
Corresponding Author. E-mail: nishananishu@soc.ku.ac.bd